
Clubfoot is a complex foot deformity present at birth, which leads to a significant functional deficit if untreated and a source of anxiety to parents. Fortunately, the deformity can be treated, and the child can lead a healthy life without residual defects.
CAUSES
There is no definitive cause seen, but it is a genetically determined (about 25% incidence if a parent has a clubfoot). It is a fairly common childhood deformity with a reported incidence of 1 in 1000 in Indian population as well.
It can be associated with various syndromes like
Arthrogryposis
Tibial hemimelia
Myelodysplasia
The syndromic clubfoot is generally rigid and requires a more extended treatment for the betterment of the child.
DEFORMITY
C – Cavus ( tightness of the intrinsic muscles)
A – Adductus
V – Varus
E – Equinus
CLINICAL FINDINGS
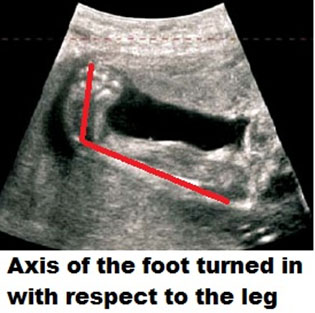
It is an easily identifiable entity, and the toes and sole of the feet point inwards. There is a collective entity called “positional” clubfoot, which primarily differs from the “structural” club foot, where the club feet are not correctable by passive forces. The positional clubfoot is mainly a packaging disorder where the foot can be passively corrected and is more due to external compression inside a tight uterus without a structural problem in the feet themselves. While in the structural club foot, there is a tight tissue tether that needs to be stretched out by constant pressure and the deformity correction obtained. Most often than not, the fully corrected foot is still going to be a little smaller than the regular foot, and it stays like that till skeletal maturity.

Presently, many clubfeet are recognized in utero during prenatal Ultrasound screening. It is an eminently treatable problem, and there is no need for anxiety for parents and individuals in its management.
TREATMENT
The primary method of treating clubfoot is by a technique called the “PONSETI” technique.
Dr. Ponseti has revolutionized the treatment of clubfoot and has been a genuinely revolutionary intervention. Before the advent of the ponseti method, many patients ended up with a painful, stiff foot in order to correct a deformity. But, with the use of this elegant method, we can obtain excellent correction with little recurrence. In an advanced country like the USA, he published his experience in 1963 in a reputed journal called “Journal of Bone and Joint Surgery.” Unfortunately, most Orthopedic surgeons did not accept his method till the late ’90s until parent groups got active on the internet and sought his expertise was in demand and now is the standard of care across the world.

PROTOCOL
The serial POP casting of the feet weekly for 6-9 casts will help to obtain correction to most of the deformity except the equinus. In 80-90% of cases, the child needs a heel cord tenotomy to correct the deformity. We undertake the tenotomy in the operating room as there is complete control, and the child is relaxed. Many club foot kids do not have a dorsalis pedis artery. If there is an inadvertent injury to the posterior tibial artery during tenotomy, it can lead to significant problems of blood flow to the foot. Operating in the clinic has been advocated by Dr. Ponseti and has been done safely in large practices.


MAINTENANCE PHASE
Post-tenotomy cast – 3 weeks
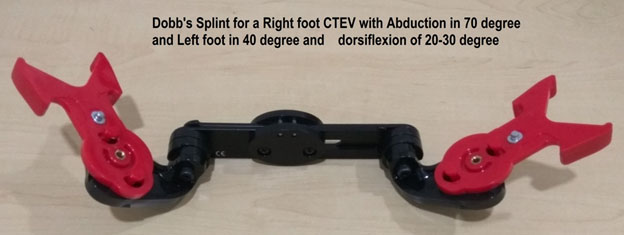
Bracing with Foot Abduction Orthosis- 22-23 hours for three months and later night time bracing for 3-4 years Dennis brown Splint/ Dobb’s splint are orthosis that helps maintain the correction of the deformity. The splints keep the affected foot in a 60-70 degree of external rotation and 20-30 degrees of dorsiflexion. The primary difference between the DB splint and the Dobb’s is the ability to move the feet independently in Dobb’s splint while both feet move together in Dennis Brown splint.
Recurrence/Relapse of Club foot
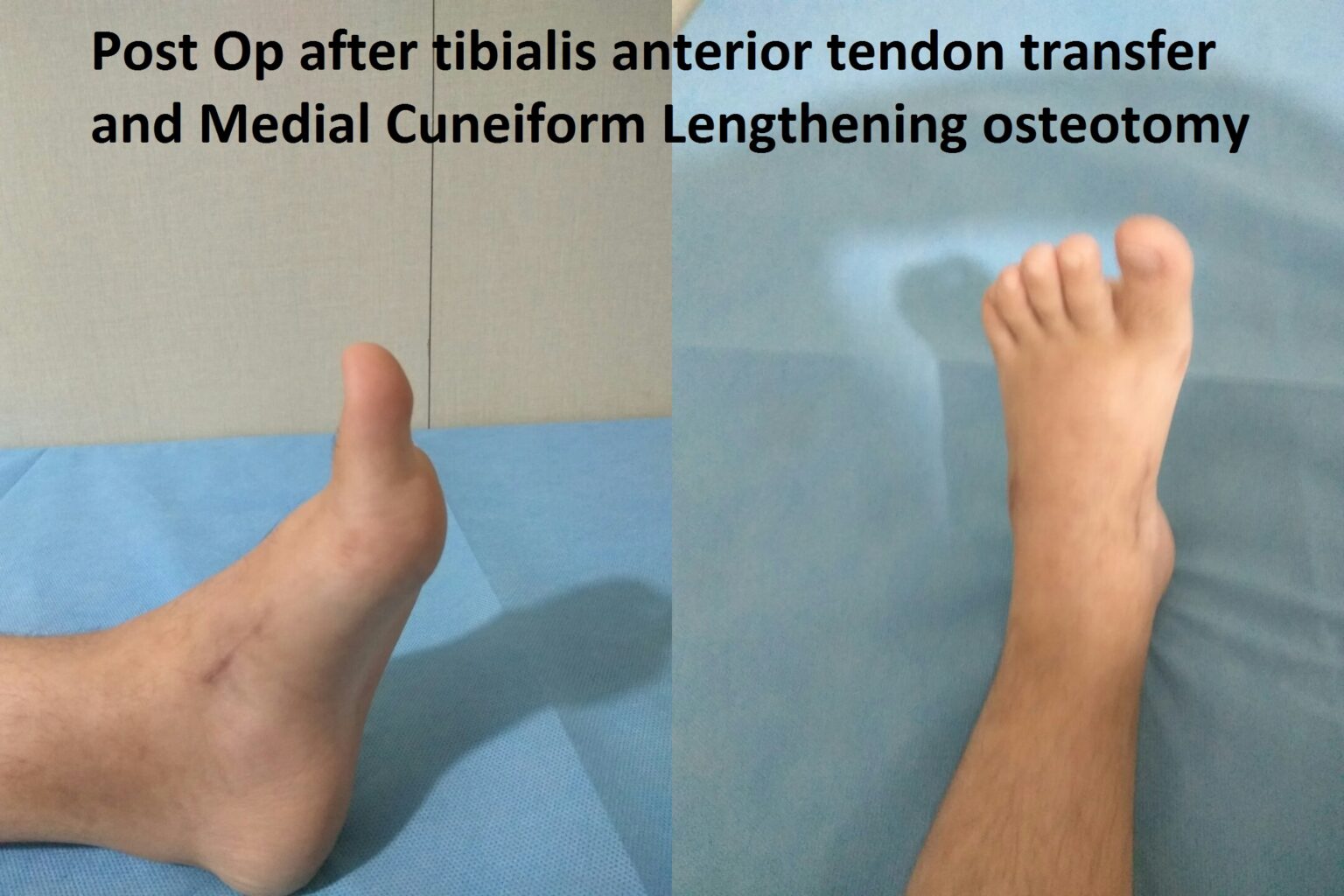
The recurrence is an unlikely phenomenon if a proper bracing protocol is followed. There could be minor relapse with dynamic supination and in-toeing when in 10-20% of patients, a Tibialis Anterior muscle transfer might be necessary.
Case Illustration
A 6-year-old girl presents with a recurrence of club foot. She developed dynamic supination and was treated with tendon transfer and medial column lengthening to get a good plantigrade foot.

Neglected Club foot
Fortunately, the incidence of neglected club foot has been reducing. The lifelong morbidity of this condition can be disabling, and the treatment for neglected club foot can be major surgeries with stiffness almost always as a complication.
